 |
|---|
หน้าหลัก | สุขภาพดี | สุภาพสตรี | การแปลผลเลือด | โรคต่างๆ | วัคซีน

ภาวะ hypertensive emergency
คือ ภาวะ ที่มีความดันโลหิตมากกว่า 180/120 mmHg โดยมีความจำเป็นที่จะต้องรีบจัดการลดระดับความดันโลหิตลงมาอย่างเร่งด่วน ปกติจะเลือกใช้การรักษาหลักแบบ ยาฉีด เช่น sodium nitropusside, nicardipine, fenoldopam เป็นต้น เนื่องจากยาสามารถออกฤทธิ์ได้อย่างรวดเร็ว มีระยะเวลาในการออกฤทธิ์สั้น และสามารถทำนายผลการตอบสนองต่อยาระหว่างที่มีการปรับขนาดยาได้ โดยปราศจากความแปรปรวนของค่าความดันโลหิต และการปรับขนาดยาไม่มากเกินความจำเป็น เพื่อให้ความดันโลหิตถึงเป้าหมาย คือ มีค่าความดันโลหิตลดลงไม่ต่ำกว่า 140/90 mmHg หรือความดันเฉลี่ยลดลงไม่เกิน 25 % ในชั่วโมงแรก และถ้าผู้ป่วยมี stable ดี สามารถลดลงเป็น 160/100 mmHg ใน 2-6 ชั่วโมงต่อมาได้ สำหรับวิธีการให้ยาจะแตกต่างไปตามชนิดของยา สำหรับยา captopril เป็นยาในกลุ่ม short-acting ACE Inhibitor ในรูปแบบ oral ซึ่งจะนิยมใช้ในภาวะ hypertensive urgency คือ มีความดันโลหิตมากกว่า 180/120 mmHg แต่ไม่มีภาวะของอวัยวะเสื่อม โดยเริ่มต้นให้ในขนาด 25-50 mg และให้ซ้ำได้ทุก 1-2 ชม. ยาออกฤทธฺ์ใน 15-30 นาที และมีระยะเวลาออกฤทธิ์นาน 2-6 ชม. สามารถสังเกตผลของความดันโลหิตในการตอบสนองต่อยาได้ภายใน 30-60 นาที
โรคความดันโลหิตสูงเป็นโรคเรื้อรังและมักจะมีการเปลี่ยนแปลงของหลอดเลือดทำให้มีการเสื่อมของวัยวะต่างๆ แต่หากมีภาวะที่ความดันโลหิตเพิ่มอย่างรวดเร็ว ซึ่งอาจจะทำให้เสี่ยงต่อผลเสียของอวัยวะ จึงเป็นภาวะความดันโลหิตสูงที่เร่งด่วนหรือฉุกเฉืนที่ต้องรีบประเมินและให้การรักษา
ภาวะเร่งด่วนของความดันโลหิตสูง Hypertensive Urgency
ภาวะเร่งด่วนของความดันโลหิตสูง
หมายถึงความดันโลหิตมากกว่า 180/110 มมปรอท ซึ่งยังไม่มีอวัยวะเสียหายวึ่งอาจจะมีหรือไม่มีอาการดังต่อไปนี้
การรักษาจะต้องมีการปรับยา หรือเพิ่มยา โดยที่อาจจะไม่ต้องนอนโรงพยาบาลเพื่อลดความดันอย่างรวดเร็ว
ภาวะฉุกเฉินจากความดันโลหิตสูง Hypertensive Emergency
หมายถึงภาวะความดันโลหิตที่สูงระดับที่จะเป็นอันตรายต่ออวัยวะ โดยทั่วไปความดันโลหิตมักจะมากกว่า 180/120 มมปรอท แต่อาจจะเกิดอวัยวะเสียหายที่ระดับความดันโลหิตต่ำกว่านี้หากคนผู้นั้นไม่เคยเป็นโรคความดันโลหิตมาก่อน
ผลของการที่ไม่สามารถควบคุมความดันโลหิตในช่วงนี้อาจจะรุนแรงและรวมถึง
หากคุณได้รับการอ่านความดันโลหิต 180 หรือสูงกว่าด้านบนหรือ 110 หรือสูงกว่าด้านล่างและมีอาการของความเสียหายที่อาจอวัยวะ (เจ็บหน้าอกหายใจถี่, ปวดหลัง, ชา / จุดอ่อนการเปลี่ยนแปลงในการมองเห็นความยากลำบากใด ๆ พูด) ไม่รอเพื่อดูว่าแรงดันของคุณลงมาในตัวเอง ขอความช่วยเหลือทางการแพทย์ฉุกเฉินทันที โทร 9-1-1 ถ้าคุณไม่สามารถเข้าถึงบริการการแพทย์ฉุกเฉิน (EMS) มีคนขับรถคุณไปโรงพยาบาลทันที
ความดันโลหิตสูงในกรณีฉุกเฉินครอบคลุมสเปกตรัมของการนำเสนอผลงานทางคลินิกในการที่ไม่สามารถควบคุมความดันเลือด (bps) นำไปสู่ความก้าวหน้าหรือความผิดปกติที่กำลังจะมาปลายอวัยวะ ในเงื่อนไขเหล่านี้, ความดันโลหิตควรจะลดลงอย่างจริงจังในช่วงนาทีถึงชั่วโมง
ความเสียหายที่ปลายอวัยวะระบบประสาทเนื่องจากไม่สามารถควบคุมความดันโลหิตอาจรวมถึงการเซ็ปความดันโลหิตสูงเกิดอุบัติเหตุหลอดเลือดสมอง / กล้ามเนื้อสมอง subarachnoid ตกเลือดและ / orintracranial ตกเลือด. [1] ความเสียหายหัวใจและหลอดเลือดปลายอวัยวะอาจรวมถึงกล้ามเนื้อหัวใจขาดเลือด / กล้ามเฉียบพลันความผิดปกติของหัวใจห้องล่างซ้ายเฉียบพลัน อาการบวมน้ำที่ปอดและ / หรือผ่า ระบบอวัยวะอื่น ๆ นอกจากนี้ยังอาจได้รับผลกระทบจากความดันโลหิตสูงที่ไม่สามารถควบคุมซึ่งอาจนำไปสู่ความล้มเหลวเฉียบพลันไต / ไม่เพียงพอ, จอประสาทตา, eclampsia หรือโรคโลหิตจาง hemolytic microangiopathic. [1]
กับการถือกำเนิดของ antihypertensives ที่อุบัติการณ์ของการเกิดเหตุฉุกเฉินความดันโลหิตสูงได้ลดลงจาก 7% เป็นประมาณ 1% ของผู้ป่วยที่มีความดันโลหิตสูง. [2] นอกจากนี้อัตราการรอดตาย 1 ปีที่เกี่ยวข้องกับสภาพนี้ได้เพิ่มขึ้นจากเพียง 20% (ก่อนที่จะ 1950) มีอัตราการอยู่รอดของกว่า 90% ด้วยการรักษาทางการแพทย์ที่เหมาะสม. [3]
ประวัติและการตรวจร่างกาย
ประวัติและการตรวจร่างกายกำหนดลักษณะความรุนแรงและการจัดการของเหตุการณ์ความดันโลหิตสูง ประวัติศาสตร์ควรมุ่งเน้นไปที่การปรากฏตัวของความผิดปกติของปลายอวัยวะสภาพแวดล้อมความดันโลหิตสูงและสาเหตุที่สามารถระบุตัวตนใด ๆ
การนำเสนอผลงานทางคลินิกพบมากที่สุดของความดันโลหิตสูงมีเหตุฉุกเฉินกล้ามสมอง (24.5%) อาการบวมน้ำที่ปอด (22.5%), ความดันโลหิตสูง encephalopathy (16.3%) หัวใจล้มเหลว andcongestive (12%) การนำเสนอผลงานทางคลินิกอื่น ๆ ที่เกี่ยวข้องกับเหตุฉุกเฉิน ได้แก่ ความดันโลหิตสูงโรคหลอดเลือดสมองแตก, ผ่าและ eclampsia [4] เช่นเดียว asacute กล้ามเนื้อหัวใจตาย
ในผู้ป่วยตั้งครรภ์วิกฤตความดันโลหิตสูงเฉียบพลันมักจะเป็นผลมาจากครรภ์เป็นพิษอย่างรุนแรงและสามารถนำไปสู่โรคหลอดเลือดสมองมารดา decompensation หัวใจ decompensation ของทารกในครรภ์ที่เกิดจากการลดลงของมดลูกปะ, abruption และตายระหว่างคลอด. [5]
ระยะเวลาและความรุนแรงของความดันโลหิตสูงมาก่อนของผู้ป่วย (รวมถึงระดับของการควบคุมความดันโลหิต) ควรมีการประเมินเช่นเดียวกับประวัติความเป็นมายาของผู้ป่วย รายละเอียดของการรักษาความดันโลหิตสูงยาเสพติดและการปฏิบัติตามการบริโภคมากกว่าที่เคาน์เตอร์ (OTC) การเตรียมการเช่นตัวแทนติกและการใช้ยาเสพติดเช่นโคเคนเป็นองค์ประกอบที่สำคัญของประวัติศาสตร์ยา นอกจากนี้ยังเป็นสิ่งสำคัญที่จะล้วงเอาข้อมูลเกี่ยวกับการปรากฏตัวของความผิดปกติก่อนหน้านี้ปลายอวัยวะไตโดยเฉพาะอย่างยิ่งและโรคหลอดเลือดสมองและปัญหาสุขภาพอื่น ๆ (เช่นโรคต่อมไทรอยด์โรค Cushing, โรคลูปัส) ในผู้ป่วยหญิง, กำหนดวันประจำเดือนของพวกเขาที่ผ่านมา
ผู้ป่วยอาจบ่นของอาการเฉพาะที่แนะนำความผิดปกติของปลายอวัยวะอาจจะนำเสนอ อาการเจ็บหน้าอกอาจบ่งบอกถึงการขาดเลือดของกล้ามเนื้อหัวใจหรือกล้ามเนื้อปวดหลังอาจหมายถึงเลือดผ่า; และหายใจลำบากอาจแนะนำอาการบวมน้ำที่ปอดหรือหัวใจล้มเหลว การปรากฏตัวของอาการทางระบบประสาทอาจรวมถึงการชักรบกวนการมองเห็นและการเปลี่ยนแปลงของระดับความรู้สึกตัวและอาจจะเป็นตัวบ่งชี้ของความดันโลหิตสูง encephalopathy
การตรวจร่างกายควรประเมินว่าความผิดปกติของปลายอวัยวะที่เป็นปัจจุบัน ความดันโลหิตไม่ควรจะวัดเพียงทั้งในท่านอนหงายและท่ายืน (ประเมินการสูญเสียปริมาณ) แต่ก็ควรจะวัดในแขนทั้งสองข้าง (ความแตกต่างอย่างมีนัยสำคัญอาจแนะนำให้ผ่า)
การปรากฏตัวของจอประสาทตาเลือดใหม่ exudates หรือ Papilledema แนะนำฉุกเฉินความดันโลหิตสูง ประเมินการปรากฏตัวของหัวใจล้มเหลวซึ่งอาจระบุอาการหลอดเลือดดำคอ, ครืดคราดในการตรวจคนไข้และอาการบวมน้ำ ระบบประสาทส่วนกลาง (CNS) ผลการวิจัยอาจรวมถึงการเปลี่ยนแปลงในระดับของผู้ป่วยของสติและสาขาภาพและ / หรือการปรากฏตัวของสัญญาณทางระบบประสาทโฟกัส ฝูงท้องหรือ bruits อาจจะตั้งข้อสังเกต
การประเมินผลของความดันโลหิตสูงที่ไม่สามารถควบคุม
ขอรับระดับอิเล็กเช่นเดียวกับวัดของยูเรียไนโตรเจนในเลือด (BUN) และระดับ creatinine ในการประเมินการด้อยค่าของไต ปัสสาวะ dipstick ในการตรวจสอบปัสสาวะหรือโปรตีนในปัสสาวะและปัสสาวะกล้องจุลทรรศน์เพื่อตรวจหาเซลล์เม็ดเลือดแดง (เม็ดเลือดแดง) หรือปลดเปลื้อง RBC ควรที่จะดำเนินการ
เซลล์เม็ดเลือดสมบูรณ์ (CBC) และละเลงเลือดควรจะได้รับการยกเว้นโรคโลหิตจาง microangiopathic และหน้าจอทางพิษวิทยา, ทดสอบการตั้งครรภ์และการทดสอบต่อมไร้ท่ออาจจะได้รับตามความจำเป็น
การถ่ายภาพควรจะกำกับโดยนำเสนอทางคลินิก หากมีหลักฐานทางคลินิกของอาการบวมน้ำที่ปอดหรือผู้ป่วยที่มีอาการเจ็บหน้าอกถ่ายภาพรังสีทรวงอกและคลื่นไฟฟ้าหัวใจจะมีการแสดง ผู้ป่วยที่มีอาการทางระบบประสาทที่ควรได้รับการประเมินด้วยการสแกนหัว CT แรกกับการถ่ายภาพขั้นสูงที่กำหนดโดยนำเสนอทางคลินิก
ความดันโลหิตสูงมะเร็ง
ความดันโลหิตสูงมะเร็งและความดันโลหิตสูงเร่งมีทั้งความดันโลหิตสูงในกรณีฉุกเฉินที่มีผลลัพธ์ที่คล้ายคลึงกันและการบำบัดรักษา ความดันโลหิตสูงมะเร็งอาจจะหรืออาจจะไม่ได้เกี่ยวข้องกับเงื่อนไขทางคลินิกอยู่ในความเร่งด่วนความดันโลหิตสูง ผู้ป่วยความดันโลหิตสูงมะเร็งมักจะมี Papilledema จอประสาทตา (เท่าที่เห็นในภาพด้านล่าง) [6] เช่นเดียวกับเลือดเปลวไฟที่มีรูปทรงและสารที่หลั่ง ลักษณะทางคลินิกอื่น ๆ ของความดันโลหิตสูงมะเร็งอาจรวมถึง encephalopathy, สับสน, ความล้มเหลวในกระเป๋าหน้าท้องซ้าย intravascular ก้อนและการทำงานของไตบกพร่องด้วยปัสสาวะและการสูญเสียน้ำหนัก
จุดเด่นทางพยาธิวิทยาของความดันโลหิตสูงมะเร็งเป็นเนื้อร้าย fibrinoid ของหลอดเลือดที่เกิดขึ้นมีระบบ แต่เฉพาะในไต ผู้ป่วยเหล่านี้พัฒนาภาวะแทรกซ้อนที่อันตรายถึงชีวิตหากได้รับการรักษาและอื่น ๆ กว่า 90% จะไม่รอดเกิน 1-2 ปี ดูความดันโลหิตสูงมะเร็ง
If you get a blood pressure reading of 180 or higher on top or 110 or higher on the bottom, and are having any symptoms of possible organ damage (chest pain, shortness of breath, back pain, numbness/weakness, change in vision, difficulty speaking) do not wait to see if your pressure comes down on its own. Seek emergency medical assistance immediately. Call 9-1-1. If you can't access the emergency medical services (EMS), have someone drive you to the hospital immediately.
Hypertensive emergencies encompass a spectrum of clinical presentations in which uncontrolled blood pressures (BPs) lead to progressive or impending end-organ dysfunction. In these conditions, the BP should be lowered aggressively over minutes to hours.
Neurologic end-organ damage due to uncontrolled BP may include hypertensive encephalopathy, cerebral vascular accident/cerebral infarction, subarachnoid hemorrhage, and/orintracranial hemorrhage.[1] Cardiovascular end-organ damage may include myocardial ischemia/infarction, acute left ventricular dysfunction, acute pulmonary edema, and/or aortic dissection. Other organ systems may also be affected by uncontrolled hypertension, which may lead to acute renal failure/insufficiency, retinopathy, eclampsia, or microangiopathic hemolytic anemia.[1]
With the advent of antihypertensives, the incidence of hypertensive emergencies has declined from 7% to approximately 1% of patients with hypertension.[2] In addition, the 1-year survival rate associated with this condition has increased from only 20% (prior to 1950) to a survival rate of more than 90% with appropriate medical treatment.[3]
History and physical examination
The history and the physical examination determine the nature, severity, and management of the hypertensive event. The history should focus on the presence of end-organ dysfunction, the circumstances surrounding the hypertension, and any identifiable etiology.
The most common clinical presentations of hypertensive emergencies are cerebral infarction (24.5%), pulmonary edema (22.5%), hypertensive encephalopathy (16.3%), andcongestive heart failure (12%). Other clinical presentations associated with hypertensive emergencies include intracranial hemorrhage, aortic dissection, and eclampsia,[4] as well asacute myocardial infarction.
In pregnant patients, acute hypertensive crisis usually results from severe preeclampsia and can lead to maternal stroke, cardiopulmonary decompensation, fetal decompensation caused by reduced uterine perfusion, abruption, and stillbirth.[5]
The duration and severity of the patient’s preexisting hypertension (including the degree of BP control) should be evaluated, as well as the patient's medication history. Details of antihypertensive drug therapy and compliance, intake of over-the-counter (OTC) preparations such as sympathomimetic agents, and use of illicit drugs such as cocaine are important elements of the medication history. In addition, it is important to elicit information about the presence of previous end-organ dysfunction, particularly renal and cerebrovascular disease, and any other medical problems (eg, thyroid disease, Cushing disease, systemic lupus). In female patients, determine the date of their last menstrual period.
Patients may complain of specific symptoms that suggest end-organ dysfunction may be present. Chest pain may indicate myocardial ischemia or infarction, back pain may denote aortic dissection; and dyspnea may suggest pulmonary edema or congestive heart failure. The presence of neurologic symptoms may include seizures, visual disturbances, and altered level of consciousness and may be indicative of hypertensive encephalopathy.
The physical examination should assess whether end-organ dysfunction is present. BP should not only be measured in both the supine position and the standing position (assess volume depletion), but it should also be measured in both arms (a significant difference may suggest aortic dissection).
The presence of new retinal hemorrhages, exudates, or papilledema suggests a hypertensive emergency. Evaluate for the presence of heart failure, which may be indicated jugular venous distention, crackles on auscultation, and peripheral edema. Central nervous system (CNS) findings may include changes in the patient's level of consciousness and visual fields, and/or the presence of focal neurologic signs. Abdominal masses or bruits may be noted.
Evaluation of uncontrolled hypertension
Obtain electrolyte levels, as well as measurements of blood urea nitrogen (BUN) and creatinine levels to evaluate for renal impairment. A dipstick urinalysis to detect hematuria or proteinuria and microscopic urinalysis to detect red blood cells (RBCs) or RBC casts should also be performed
A complete blood cell (CBC) and peripheral blood smear should be obtained to exclude microangiopathic anemia, and a toxicology screen, pregnancy test, and endocrine testing may be obtained, as needed.
Imaging should be directed by clinical presentation. If there is clinical evidence of pulmonary edema or the patient has chest pain, chest radiography and ECG are indicated. Patients with neurological signs should be evaluated with a head CT scan initially, with more advanced imaging determined by clinical presentation.
Malignant hypertension
Malignant hypertension and accelerated hypertension are both hypertensive emergencies, with similar outcomes and therapies. Malignant hypertension may or may not be associated with clinical conditions present in hypertensive urgency. A patient with malignant hypertension always has retinal papilledema (as seen in the image below),[6] as well as flame-shaped hemorrhages and exudates. Other clinical features of malignant hypertension may include encephalopathy, confusion, left ventricular failure, intravascular coagulation, and impaired renal function, with hematuria and weight loss.
The pathologic hallmark of malignant hypertension is fibrinoid necrosis of the arterioles, which occurs systemically, but specifically in the kidneys. These patients develop fatal complications if untreated, and more than 90% will not survive beyond 1-2 years. See Malignant Hypertension.
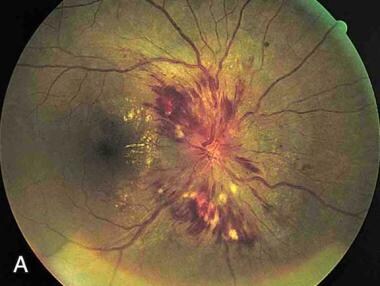 Papilledema. Note the swelling of the optic disc, with blurred margins
Papilledema. Note the swelling of the optic disc, with blurred marginsA study by Amraoui et al found a higher all-cause mortality rate in patients with malignant hypertension than in persons who were normotensive or hypertensive, even though the cardiovascular risk profile for the malignant hypertension patients was more favorable than that for the hypertensive controls. The study, which compared 120 patients with a history of malignant hypertension with 120 normotensive and 120 hypertensive persons, found that the malignant hypertension patients had lower total cholesterol, low-density lipoprotein cholesterol, and body mass index values than did the hypertensive controls. However, the median estimated glomerular filtration rate was higher in the normotensive and hypertensive controls than in the malignant hypertension group. Annual all-cause mortality per 100 patient-years was 2.6 for the patients with malignant hypertension, compared with 0.2 and 0.5 for the normotensive and hypertensive controls, respectively.[7]
To see complete information on hypertension, please go to the main article by clicking here.
Management of Hypertensive Emergencies
Approximately 3-45% of adult patients have at least one incident of increased BP during their stay in the emergency department (ED). The fundamental principle in determining the necessary ED care of the hypertensive patient is the presence or absence of end-organ dysfunction. Many patients present to the ED with elevated BPs; however, only a small proportion of patients will require emergency treatment. An important point to remember in the management of the patient with any degree of BP elevation is to "treat the patient and not the number."
The primary goal of the emergency physician is to determine which patients with acute hypertension are exhibiting symptoms of end-organ damage and require immediate intravenous (IV) parenteral therapy. In contrast, patients presenting with acutely elevated BP (systolic BP [SBP] >200 mm Hg or diastolic BP [DBP] >120 mm Hg) without symptoms and whose BP stays significantly elevated to this level on discharge should have initiation of medical therapy and close follow-up in the outpatient setting.[8]
Thus, optimal control of hypertensive situations balances the benefits of immediate decreases in BP against the risk of a significant decrease in target organ perfusion. The emergency physician must be capable of appropriately evaluating patients with an elevated BP, correctly classifying the hypertension, determining the aggressiveness and timing of therapeutic interventions, and making disposition decisions.
Acutely lowering BP in the ED for clinical situations other than those listed below is controversial and generally should be avoided.
Pharmacotherapy
Optimal pharmacotherapy is dependent upon the specific organ at risk (see individual sections below). In patients presenting with hypertensive emergencies, antihypertensive drug therapy has been shown to be effective in acutely decreasing blood pressure.[9]
Sodium nitroprusside is a commonly used medication. It is a short-acting agent, and the BP response can be titrated from minute to minute. However, patients must have constant monitoring in an intensive care unit. The potential exists for thiocyanate and cyanide toxicity with prolonged use or if the patient has renal or hepatic failure.
Labetalol, an alfa- and beta-blocking agent, has proven to be quite beneficial in the treatment of patients with hypertensive emergencies. Labetalol is particularly preferred in patients with acute dissection and patients with end-stage renal disease. Boluses of 10-20 mg may be administered, or the drug may be infused at 1 mg/min until the desired BP is obtained. Once an adequate BP level is obtained, oral hypertensive therapy should be initiated, and patients are gradually weaned from parenteral agents.
Fenoldopam, a peripheral dopamine-1-receptor agonist is given as initial IV dose of 0.1 µg/kg/min titrated every 15 minutes.
Clevidipine, a dihydropyridine calcium channel blocker, is administered intravenously for rapid and precise BP reduction.[10] It is rapidly metabolized in the blood and tissues and does not accumulate in the body. Initiate IV infusion of clevidipine at 1-2 mg/h; titrate the dose at short intervals (ie, 90 s) initially by doubling the dose.
As the BP approaches its goal, increase the clevidipine dose by less than double, and lengthen the time between dose adjustments to every 5-10 minutes. An approximately 1-2 mg/h increase produces an additional 2-4 mm Hg decrease in SBP. Typically, the therapeutic response is achieved with 4-6 mg/h, although severe hypertension may require higher doses. Most patients have received maximum doses of 16 mg/h or less; experience is limited with short-term dosing as high as 32 mg/h. Because of lipid load restrictions, do not exceed 1000 mL or an average of 21 mg/h within a 24-hour period; experience is limited with use beyond 72 hours.
Neurologic emergencies
Rapid BP reduction is indicated in neurologic emergencies, such as hypertensive encephalopathy, acute ischemic stroke, acute intracerebral hemorrhage, and subarachnoid hemorrhage.
In hypertensive encephalopathy, the treatment guidelines are to reduce the MAP 25% over 8 hours.[11] Labetalol,nicardipine, esmolol are the preferred medications; nitroprusside and hydralazine should be avoided.
For acute ischemic stroke, the preferred medications are labetalol and nicardipine. Withhold antihypertensive medications unless the SBP is >220 mm Hg or the DBP is >120 mm Hg, UNLESS the patient is receiving IV or intra-arterial (IA) fibrinolysis; then, the goal BP is an SBP of < 185 mm Hg and DBP < 110 mm Hg. After treatment with fibrinolysis, the SBP should be maintained < 180 mm Hg and the DBP at < 105 mm Hg for 24 hours.[11]
For acute intracerebral hemorrhage, the preferred medications are labetalol, nicardipine, and esmolol; avoid nitroprusside and hydralazine. The treatment is based on clinical/radiographic evidence of increased intracranial pressure (ICP). If there are signs of increased ICP, maintain the MAP just below 130 mm Hg (or SBP < 180 mm Hg) for the first 24 hours after onset. In patients without increased ICP, maintain the MAP < 110 mm Hg (or SBP < 160 mm Hg) for the first 24 hours after symptom onset.[11]
Recent evidence shows that in cases of acute intracerebral hemorrhage, early intensive BP control is well tolerated and can reduce hematoma growth in patients treated within 6 hours after the onset of intracerebral hemorrhage.[12, 13] The target systolic pressure for these studies was 140 mm Hg and routine IV medications were used. The target SBP was maintained over 7 days.[12, 13]
In subarachnoid hemorrhage, nicardipine, labetalol, and esmolol are also the preferred agents; again, nitroprusside and hydralazine should be avoided. Maintain the SBP < 160 mm Hg until the aneurysm is treated or cerebral vasospasm occurs. Although oral nimodipine is used to prevent delayed ischemic neurologic deficits, it is NOT indicated for treating acute hypertension.[11]
Cardiovascular emergencies
Rapid BP reduction is also indicated in cardiovascular emergencies, such as aortic dissection, acute coronary syndrome, and acute heart failure.
In aortic dissection, the preferred medications are labetalol, nicardipine, nitroprusside (with beta-blocker), esmolol, andmorphine sulfate. However, avoid beta-blockers if there is aortic valvular regurgitation or suspected cardiac tamponade. Maintain the SBP at < 110 mm Hg, unless signs of end-organ hypoperfusion are present. The preferred treatment includes a combination of narcotic analgesics (morphine sulfate), beta blockers (labetalol, esmolol), and vasodilators (nicardipine, nitroprusside). Calcium channel blockers (verapamil, diltiazem) are an alternative to beta blockers.[14]
For acute coronary syndrome, beta blockers and nitroglycerin are the preferred drugs. Treatment is indicated if the SBP is >160 mm Hg and/or the DBP is >100 mm Hg. Reduce the BP by 20-30% of baseline. Note that thrombolytics are contraindicated if the BP is >185/100 mm Hg.[15]
In acute heart failure, the preferred medications are IV nitroglycerin or sublingual nitroglycerin and IV enalaprilat. Treat with vasodilators (in addition to diuretics) for a SBP =140 mm Hg.[15]
Cocaine toxicity/pheochromocytoma
Diazepam, phentolamine, and nitroglycerin/nitroprusside are the preferred drugs. However, avoid beta-adrenergic antagonists before administering phentolamine.
Hypertension and tachycardia from cocaine toxicity rarely require specific treatment. alfa-adrenergic antagonists (phentolamine) are the preferred agents for cocaine-associated acute coronary syndromes.[16]Pheochromocytoma treatment guidelines are similar to that of cocaine toxicity. Only after alfa blockade can beta blockers be added for BP control.
Preeclampsia/eclampsia
The preferred medications are hydralazine, labetalol, and nifedipine. Avoid - Nitroprusside, angiotensin-converting enzyme inhibitors, esmolol. In women with eclampsia or preeclampsia, the SBP should be < 160 mm Hg and the DBP should be < 110 mm Hg in the antepartum and intrapartum periods. If the platelet count is less than 100,000 cells mm3, the BP should be maintained below 150/100 mm Hg. Patients with eclampsia or preeclampsia should also be treated with IVmagnesium sulfate to avoid seizures.[17]
Perioperative hypertension
Nitroprusside, nitroglycerin, and esmolol are preferred. Target the perioperative BP to within 20% of the patient's baseline pressure, except if there is the potential for life-threatening arterial bleeding. Perioperative beta blockers are the first choice in patients undergoing vascular procedures or in patients with an intermediate or high risk of cardiac complications.[14]
การศึกษาโดย Amraoui et al, พบอัตราการตายจากทุกสาเหตุที่สูงขึ้นในผู้ป่วยที่มีความดันโลหิตสูงมะเร็งกว่าในบุคคลที่มีความดันโลหิตสูงและโลหิตปกติแม้ว่ารายละเอียดความเสี่ยงโรคหัวใจและหลอดเลือดสำหรับผู้ป่วยความดันโลหิตสูงมะเร็งที่ดีขึ้นกว่าที่สำหรับการควบคุมความดันโลหิตสูง การศึกษาซึ่งเมื่อเทียบกับผู้ป่วยที่ 120 ที่มีประวัติความดันโลหิตสูงมะเร็งโลหิตปกติ 120 และ 120 คนความดันโลหิตสูงที่พบว่าผู้ป่วยความดันโลหิตสูงมะเร็งมีคอเลสเตอรอลรวม, ความหนาแน่นต่ำไลโปโปรตีนคอเลสเตอรอลและค่าดัชนีมวลกายกว่าการควบคุมความดันโลหิตสูง อย่างไรก็ตามค่าเฉลี่ยประมาณอัตราการกรองของไตเป็นที่สูงขึ้นในการควบคุมความดันโลหิตสูงและโลหิตปกติกว่าในกลุ่มความดันโลหิตสูงมะเร็ง ประจำปีทุกสาเหตุการตายของผู้ป่วยต่อ 100 ปีเป็น 2.6 สำหรับผู้ป่วยความดันโลหิตสูงมะเร็งเมื่อเทียบกับ 0.2 และ 0.5 สำหรับการควบคุมความดันโลหิตสูงโลหิตปกติและตามลำดับ. [7]
เพื่อดูข้อมูลที่สมบูรณ์เกี่ยวกับความดันโลหิตสูง, โปรดไปที่บทความหลักโดยคลิกที่นี่
การจัดการของความดันโลหิตสูงกรณีฉุกเฉิน
ประมาณ 3-45% ของผู้ป่วยผู้ใหญ่ที่มีอย่างน้อยหนึ่งเหตุการณ์ที่เกิดขึ้นของการเพิ่มขึ้นของ BP ระหว่างการเข้าพักของพวกเขาในแผนกฉุกเฉิน (ED) หลักการพื้นฐานในการกำหนดดูแล ED ที่จำเป็นของผู้ป่วยความดันโลหิตสูงคือการมีหรือไม่มีความผิดปกติของปลายอวัยวะ ผู้ป่วยจำนวนมากในปัจจุบันเอ็ดกับ bps สูง; แต่เพียงส่วนเล็ก ๆ ของผู้ป่วยที่จะต้องมีการรักษาฉุกเฉิน จุดสำคัญที่ต้องจำไว้ในการบริหารจัดการของผู้ป่วยที่มีระดับของความดันโลหิตระดับความสูงใด ๆ คือการ "รักษาผู้ป่วยและไม่ได้จำนวน."
เป้าหมายหลักของการแพทย์ฉุกเฉินคือการตรวจสอบว่าผู้ป่วยที่มีความดันโลหิตสูงเฉียบพลันจะแสดงอาการของความเสียหายที่ปลายอวัยวะและจำเป็นต้องใช้ทันที (IV) การบำบัดหลอดเลือด ในทางตรงกันข้ามผู้ป่วยที่มีความรุนแรงสูง BP (systolic BP [SBP]> 200 มิลลิเมตรปรอทหรือความดันโลหิต diastolic [DBP]> 120 มิลลิเมตรปรอท) โดยไม่มีอาการและการที่มีความดันโลหิตยังคงสูงขึ้นอย่างมีนัยสำคัญในระดับนี้ในการปล่อยควรจะมีการเริ่มต้นของการรักษาทางการแพทย์และ ใกล้ติดตามในการตั้งค่าผู้ป่วยนอก. [8]
ดังนั้นการควบคุมที่ดีที่สุดของสถานการณ์ความดันโลหิตสูงสมดุลประโยชน์ของการลดลงทันทีใน BP กับความเสี่ยงของการลดลงอย่างมีนัยสำคัญในเลือดไปเลี้ยงอวัยวะเป้าหมาย แพทย์ฉุกเฉินจะต้องมีความสามารถในการที่เหมาะสมในการประเมินผู้ป่วยที่มีการยกระดับความดันโลหิตอย่างถูกต้องแบ่งประเภทของความดันโลหิตสูง, การกำหนดความก้าวร้าวและระยะเวลาของการแทรกแซงการรักษาและการตัดสินใจจำหน่าย
อย่างรุนแรงลดความดันโลหิตใน ED สำหรับสถานการณ์ทางคลินิกอื่นนอกเหนือจากที่ระบุไว้ด้านล่างเป็นที่ถกเถียงและโดยทั่วไปควรหลีกเลี่ยง
การรักษาด้วยยา
ยาที่เหมาะสมขึ้นอยู่กับอวัยวะที่เฉพาะเจาะจงที่มีความเสี่ยง (ดูแต่ละส่วนด้านล่าง) ในผู้ป่วยที่มีความดันโลหิตสูงในกรณีฉุกเฉิน, การรักษาด้วยยาลดความดันโลหิตได้รับการแสดงที่จะมีประสิทธิภาพในการลดลงอย่างรุนแรงความดันโลหิต. [9]
โซเดียม nitroprusside เป็นยาที่ใช้กันทั่วไป มันเป็นตัวแทนที่ออกฤทธิ์สั้นและการตอบสนองต่อความดันโลหิตสามารถปรับขนาดโดยนาที อย่างไรก็ตามผู้ป่วยจะต้องมีการตรวจสอบอย่างต่อเนื่องในหน่วยดูแลเข้ม ที่มีศักยภาพที่มีอยู่สำหรับความเป็นพิษ thiocyanate และไซยาไนด์กับการใช้งานเป็นเวลานานหรือถ้าผู้ป่วยมีภาวะไตวายหรือตับ
Labetalol ตัวแทนอัลฟาและเบต้าบล็อกได้พิสูจน์ให้เป็นประโยชน์มากในการรักษาผู้ป่วยที่มีความดันโลหิตสูงในกรณีฉุกเฉิน Labetalol เป็นที่ต้องการโดยเฉพาะอย่างยิ่งในผู้ป่วยที่มีการผ่าเฉียบพลันและผู้ป่วยที่มีโรคไตวายเรื้อรังระยะสุดท้าย boluses 10-20 มิลลิกรัมอาจจะบริหารหรือยาเสพติดอาจจะ infused วันที่ 1 มก. / นาทีจนกว่าความดันโลหิตที่ต้องการจะได้รับ เมื่อระดับความดันโลหิตที่เพียงพอจะได้รับการรักษาด้วยความดันโลหิตสูงในช่องปากควรจะเริ่มต้นและผู้ป่วยจะค่อยๆหย่านมจากตัวแทนหลอดเลือด
Fenoldopam, อุปกรณ์ต่อพ่วงตัวเอก dopamine-1-รับจะได้รับเป็นยา IV เริ่มต้นที่ 0.1 ไมโครกรัม / กก. / นาทีปรับขนาดทุก 15 นาที
Clevidipine, ป้องกัน dihydropyridine แคลเซียมแชนแนล, เป็นยาฉีดเข้าเส้นเลือดดำสำหรับอย่างรวดเร็วและแม่นยำลดความดันโลหิต. [10] มันถูกเผาผลาญอย่างรวดเร็วในเลือดและเนื้อเยื่อและไม่เกิดการสะสมในร่างกาย เริ่มต้นที่สี่ของการแช่ clevidipine ที่ 1-2 มก. / เอช; ไทเทรตยาในช่วงเวลาสั้น ๆ (เช่น 90 s) ครั้งแรกโดยการเพิ่มปริมาณ
ในฐานะที่เป็นความดันโลหิตแนวทางเป้าหมายเพิ่มปริมาณ clevidipine โดยน้อยกว่าคู่และยืดระยะเวลาระหว่างการปรับขนาดยาทุก 5-10 นาที ประมาณ 1-2 มก. / ชมเพิ่มขึ้นก่อให้เกิดการลดลง 2-4 มิลลิเมตรปรอทเพิ่มเติมใน SBP โดยปกติแล้วการตอบสนองต่อการรักษาที่จะประสบความสำเร็จกับ 4-6 mg / H, แม้ว่าความดันโลหิตสูงอย่างรุนแรงอาจจำเป็นต้องมีปริมาณที่สูงขึ้น ผู้ป่วยส่วนใหญ่ได้รับในปริมาณที่สูงสุดถึง 16 มก. / ชั่วโมงหรือน้อยกว่า ประสบการณ์จะถูก จำกัด ด้วยการใช้ยาในระยะสั้นสูงที่สุดเท่าที่ 32 มก. / ชั่วโมง เนื่องจากข้อ จำกัด ของการโหลดไขมันไม่เกิน 1,000 มิลลิลิตรหรือเฉลี่ย 21 มิลลิกรัม / ชั่วโมงภายในระยะเวลา 24 ชั่วโมง; ประสบการณ์ที่มีข้อ จำกัด ที่มีการใช้เกิน 72 ชั่วโมง
เหตุฉุกเฉินทางระบบประสาท
ลดความดันโลหิตอย่างรวดเร็วถูกระบุในกรณีฉุกเฉินทางระบบประสาทเช่น encephalopathy ความดันโลหิตสูง, โรคหลอดเลือดสมองตีบเฉียบพลันตกเลือด intracerebral เฉียบพลันและ subarachnoid ตกเลือด
ความดันโลหิตสูงใน encephalopathy แนวทางการรักษาเพื่อลดแผนที่ 25% ในช่วง 8 ชั่วโมง [11] Labetalol, nicardipine, esmolol ยาที่ต้องการ. nitroprusside และ hydralazine ควรหลีกเลี่ยง
สำหรับโรคหลอดเลือดสมองตีบเฉียบพลันยาที่แนะนำที่มี labetalol และ nicardipine ระงับการจ่ายยาลดความดันโลหิตเว้นแต่เป็น SBP> 220 มิลลิเมตรปรอทหรือ DBP เป็น> 120 มิลลิเมตรปรอทเว้นแต่ผู้ป่วยจะได้รับ IV หรือภายในหลอดเลือดแดง (IA) การละลายลิ่มเลือด; แล้วความดันโลหิตเป้าหมายเป็น SBP ของ <185 มิลลิเมตรปรอทและ DBP <110 มิลลิเมตรปรอท หลังการรักษาด้วยการละลายลิ่มเลือดที่ SBP ควรจะรักษา <180 มิลลิเมตรปรอทและ DBP ที่ <105 มิลลิเมตรปรอทเป็นเวลา 24 ชั่วโมง. [11]
สำหรับอาการตกเลือด intracerebral เฉียบพลันยาที่แนะนำที่มี labetalol, nicardipine และ esmolol; หลีกเลี่ยงการ nitroprusside และ hydralazine การรักษาจะขึ้นอยู่กับหลักฐานทางคลินิก / ภาพรังสีของความดันในสมองเพิ่มขึ้น (ICP) หากมีสัญญาณของการเพิ่มขึ้น ICP รักษาแผนที่ด้านล่าง 130 มิลลิเมตรปรอท (หรือ SBP <180 มิลลิเมตรปรอท) สำหรับ 24 ชั่วโมงแรกหลังจากเริ่มมีอาการ ในผู้ป่วยโดยไม่ต้องเพิ่มขึ้น ICP รักษาแผนที่ <110 มิลลิเมตรปรอท (หรือ SBP <160 มิลลิเมตรปรอท) สำหรับ 24 ชั่วโมงแรกหลังจากเริ่มมีอาการ. [11]
หลักฐานล่าสุดแสดงให้เห็นว่าในกรณีของการตกเลือด intracerebral เฉียบพลันต้นการควบคุมความดันโลหิตอย่างเข้มข้นเป็นที่ยอมรับเป็นอย่างดีและสามารถลดการเจริญเติบโตของเลือดในผู้ป่วยที่ได้รับการรักษาภายใน 6 ชั่วโมงหลังจากที่เริ่มมีอาการของการตกเลือด intracerebral ได้. [12, 13] ความดันซิสโตลิเป้าหมายสำหรับการศึกษาเหล่านี้เป็น 140 มิลลิเมตรปรอทและยา IV ประจำถูกนำมาใช้ SBP เป้าหมายถูกเก็บรักษาไว้ในช่วง 7 วัน. [12, 13]
ใน subarachnoid ตกเลือด nicardipine, labetalol และ esmolol นอกจากนี้ยังมีตัวแทนที่ต้องการ; อีกครั้ง nitroprusside และ hydralazine ควรหลีกเลี่ยง รักษา SBP <160 มิลลิเมตรปรอทจนถึงปากทางได้รับการปฏิบัติหรือ vasospasm สมองเกิดขึ้น แม้ว่า nimodipine ในช่องปากจะใช้ในการป้องกันไม่ให้เกิดความล่าช้าการขาดดุลทางระบบประสาทขาดเลือดก็ไม่ได้ระบุไว้สำหรับการรักษาความดันโลหิตสูงเฉียบพลัน. [11]
กรณีฉุกเฉินโรคหัวใจและหลอดเลือด
ลดลงอย่างรวดเร็ว BP ยังได้ถูกระบุในกรณีฉุกเฉินโรคหัวใจและหลอดเลือดเช่นผ่า, โรคหลอดเลือดหัวใจเฉียบพลันและภาวะหัวใจล้มเหลวเฉียบพลัน
ในเลือดผ่ายาที่แนะนำที่มี labetalol, nicardipine, nitroprusside (Beta-Blocker) esmolol, andmorphine ซัลเฟต แต่หลีกเลี่ยงการปิดกั้นเบต้าถ้ามีสำรอกลิ้นหลอดเลือดหรือสงสัยว่าหัวใจถูกบีบรัด รักษา SBP ที่ <110 มิลลิเมตรปรอทเว้นแต่สัญญาณของ hypoperfusion ปลายอวัยวะที่มีอยู่ การรักษาที่แนะนำรวมถึงการรวมกันของยาแก้ปวดยาเสพติด (มอร์ฟีนซัลเฟต) เบต้าอัพ (labetalol, esmolol) และ vasodilators A (nicardipine, nitroprusside) แคลเซียมแชนแนลบล็อกเกอร์ (verapamil, diltiazem) เป็นทางเลือกให้กับเบต้าอัพ. [14]
สำหรับโรคหลอดเลือดหัวใจเฉียบพลัน, เบต้าอัพและไนโตรกลีเซอยาเสพติดที่ต้องการ การรักษาจะต้องระบุถ้าเป็น SBP> 160 มิลลิเมตรปรอทและ / หรือ DBP เป็น> 100 มิลลิเมตรปรอท ลดความดันโลหิตโดย 20-30% ของพื้นฐาน โปรดทราบว่า thrombolytics มีข้อห้ามถ้าความดันโลหิต> 185/100 มิลลิเมตรปรอท. [15]
หัวใจล้มเหลวเฉียบพลันยาที่แนะนำเป็นไนโตรกลีเซอ IV หรือไนโตรกลีเซอลิ้นและ IV enalaprilat การรักษาด้วย vasodilators (นอกเหนือจาก diuretics) สำหรับ SBP = 140 มิลลิเมตรปรอท. [15]
ความเป็นพิษโคเคน / pheochromocytoma
กล่อม phentolamine และไนโตรกลีเซอ / nitroprusside ยาเสพติดที่ต้องการ แต่ควรหลีกเลี่ยงคู่อริเบต้า adrenergic ก่อนที่จะบริหาร phentolamine
ความดันโลหิตสูงและหัวใจเต้นเร็วจากความเป็นพิษโคเคนไม่ค่อยต้องมีการรักษาที่เฉพาะเจาะจง คู่อริ alfa-adrenergic (phentolamine) เป็นตัวแทนที่แนะนำสำหรับโคเคนที่เกี่ยวข้องอาการหัวใจวายเฉียบพลัน. [16] แนวทางการรักษา pheochromocytoma มีความคล้ายคลึงกับที่ของความเป็นพิษโคเคน แต่หลังจากที่อัลฟาด่านสามารถเบต้าอัพเพิ่มสำหรับการควบคุมความดันโลหิต
Preeclampsia / eclampsia
ยาที่แนะนำมี hydralazine, labetalol และ nifedipine ควรหลีกเลี่ยง - nitroprusside, angiotensin แปลงสารยับยั้งเอนไซม์ esmolol ในสตรีที่มีครรภ์หรือ eclampsia ที่ควรจะ SBP <160 มิลลิเมตรปรอทและ DBP ควรจะ <110 มิลลิเมตรปรอทในงวด antepartum และคลอด ถ้านับเกล็ดเลือดน้อยกว่า 100,000 เซลล์ mm3, ความดันโลหิตควรจะรักษาด้านล่าง 150/100 มิลลิเมตรปรอท ผู้ป่วยที่มี eclampsia หรือครรภ์เป็นพิษควรที่จะรับการรักษาด้วย IVmagnesium ซัลเฟตเพื่อหลีกเลี่ยงการชัก. [17]
ความดันโลหิตสูงผ่าตัด
nitroprusside, ไนโตรกลีเซอและ esmolol เป็นที่ต้องการ เป้าหมายผ่าตัด BP ไปภายใน 20% ของความดันพื้นฐานของผู้ป่วยยกเว้นกรณีที่มีศักยภาพในการคุกคามชีวิตเลือดออกเลือดแดง เบต้าอัผ่าตัดเป็นตัวเลือกแรกในผู้ป่วยที่ขั้นตอนของหลอดเลือดหรือในผู้ป่วยที่มีความเสี่ยงสูงกลางหรือภาวะแทรกซ้อนของหัวใจ. [14]